Prof. Giammaria Fiorentini of the Department of Onco-Hematology of Azienda Ospedaliera Marche Nord, Pesaro, Italy, presented at the 35th Annual Conference of the International Clinical Hyperthermia Society (ICHS) in Guangzhou, the results of their work in the treatment with Hyperthermia (Oncothermia) in patients with brain tumors.
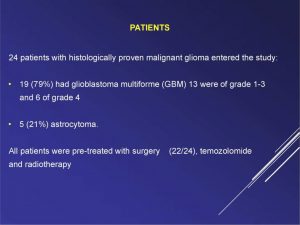
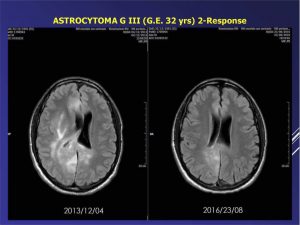
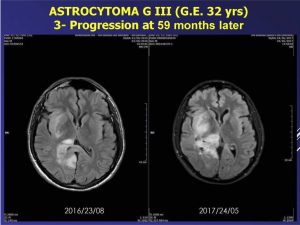
The study was carried out with an Oncotherm EHY-2000 PLUS device, on 24 patients: 19 with glioblastoma multiforme and 5 with astrocytoma. All of them were previously treated with surgery, TMZ chemotherapy and radiotherapy.
Through the article Prof. Giammaria Fiorentini describes the characteristics of brain tumors, their incidence and mortality, survival and conventional therapies that are used, with an emphasis on the case of Glioblastoma and the benefits obtained by applying Electro-hyperthermia.
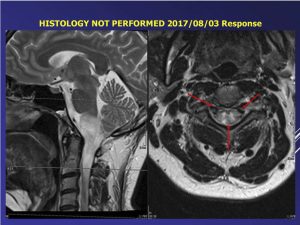
According to his observations Oncothermia (Electro-hyperthermia) is a non-invasive treatment, without toxicity and feasible to treat recurrent malignant gliomas, which allows to increase the response to the tumor and the survival of the patient.
The full article can be accessed by visiting this link.
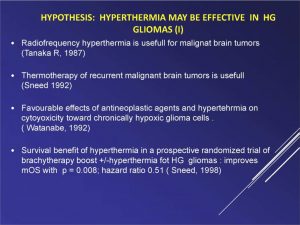
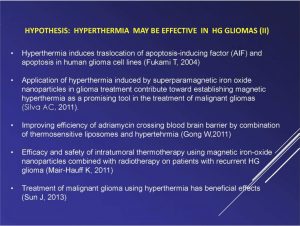
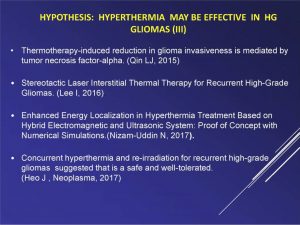
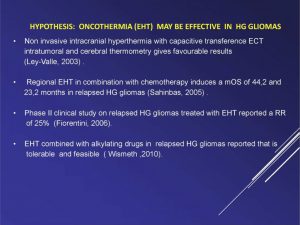
Hypothesis: Studies that observe the effectiveness of Hyperthermia in HG Gliomas.
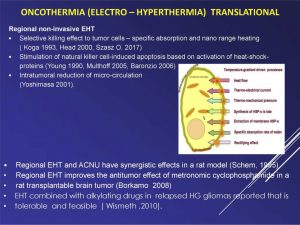
Oncothermia (Electro – Hyperthermia) traslational studies.
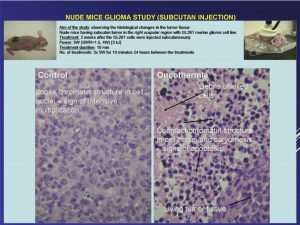
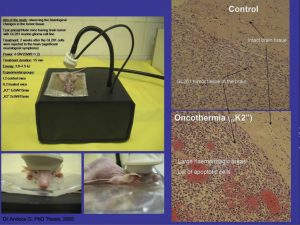
Oncothermia application in malignant gliomas.
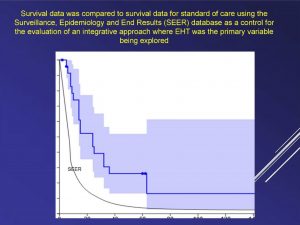
Study on the activity and toxicity of Oncothermia in recurrent malignant gliomas.
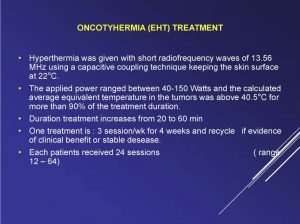
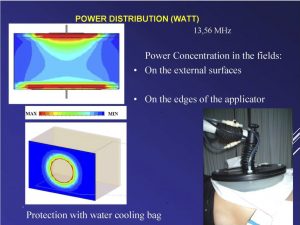
Description of the equipment used: Oncotherm EHY-2000 PLUS, non-ionizing therapy that elevates the temperature of the tumor macro and micro-enviroments, to a range of 40-45ºC, generating a 40-150 Watt radiofrequency, at 13.56 MHz.
24 patients, 19 with glioblastoma multiforme and 5 with astrocytoma. All patient were pre-treated with surgery, chemotherapy and radiotherapy.
Oncothermia treatment: 3 sessions/week for 4 weeks, 20 a 60 minutes each session.

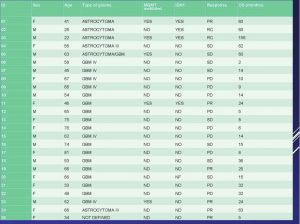
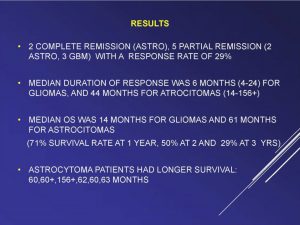
Results: 2 complete remissions and 5 partial remissions were observed. The medial OS was 14 months for gliomas and 61 months for astrocitomas.



Conclussions:
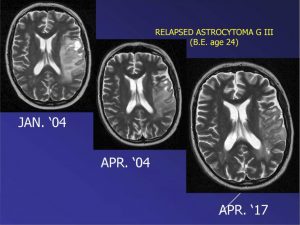
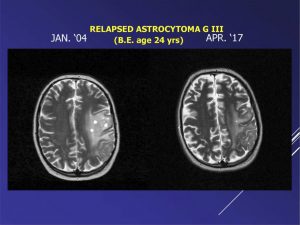
– Oncothermia applicated in patients with relapsed malignant gliomas is feasible and may increase tumor response and survival.
– EHT is a non-invasive method to treat malignant gliomas without toxicity.
– EHT appears to have effectiveness and further studies are warranted.
– EHT can be considered a landmark stone of integrative oncology.
Source:
Fiorentini G. (2018): Oncothermia in brain tumours; Oncothermia Journal 22: 151-177
www.oncothermia- journal.com/journal/2018/Oncothermia_in_brain_tumours.pdf

 Oncothermia in combination with Radiotherapy exerts a radiosensitizing effect in lung cancer.
Oncothermia in combination with Radiotherapy exerts a radiosensitizing effect in lung cancer.