Artícle written by Giammaria Fiorentini, Donatella Sarti, Virginia Casadei, Caterina Fiorentini
Onco-Ematology Department, Azienda Ospedaliera “Ospedati Riuniti Marche Nord”, 61122 Pesaro, italy
Department of Medical Biothecnologies, Division of Cardiology, University of Siena, 53100 Siena, Italy,
Presented at 36º ICHS, Budapest, 2018
Background and aims:
There has been a significant improvement in the development and application of hyperthermia treatment and there is a continuous interest and ongoing clinical research in the field of hyperthermia. This study aim to evaluate the efficacy in terms of tumor response, pain reduction and improvement of quality of life due to modulated electro- hyperthermia
(mEHT), for the treatment of cancer.
Methods
This was a retrospective observational clinical study. Patients were included in the study if they had >18 years, informed consent signed, indication for treatment with mEHT.
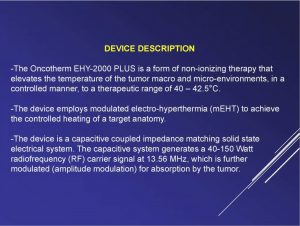
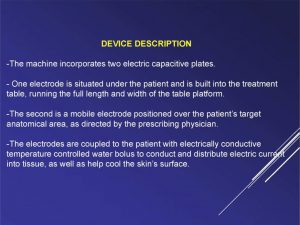
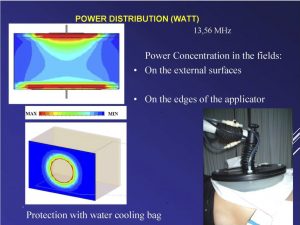
Hyperthermia was performed with short radiofrequency waves of 13.56 MHz using a capacitive coupling technique keeping the skin surface at 26 C°. The applied power ranged between 40-150 Watts and the calculated average equivalent temperature in the tumors was above 41,5 C° for more than 90% of the treatment duration (20-60 minutes gradually).
Results
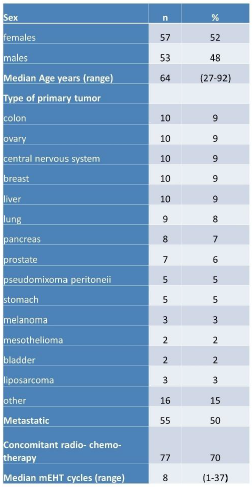
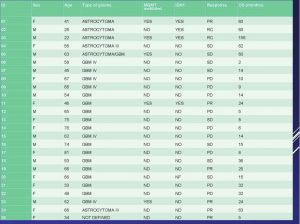
Characteristics of patients
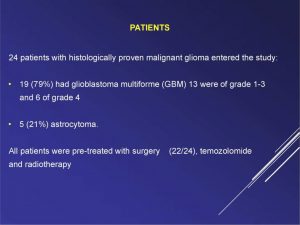
110 consecutive patients were enrolled in the study, tumor distribution was: 11 (10%) colon, 11 (10%), ovary, 10 (9%) central nervous system, 10 (9%) breast, 10 (9%) liver (cholangiocarcinoma and HCC), 10 (9%) lung, 9 (8%) pancreas, 8 (7%) prostate, 5 (5%) pseudo mixoma peritoneii, 5 (5%) stomach, 4 (5%) melanoma, 2(2%) mesothelioma, 3(3%) bladder, 3 (3%) liposarcome and 11 (10%) other type of tumor. Other chracteristics of the
sample were: 50% presence of metastasis, 70% received concomitant radio or chemotherapy and median number of mEHT cycles was 8 (range 1-37).
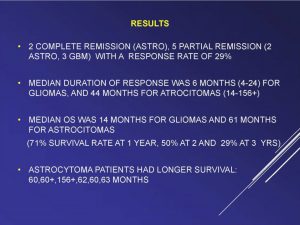
Tumor response analysis three months after mEHT showed 3% complete remission and 41% partial remission, 31 % of stable disease and 25% of progression. Median pain intensity and quality of life improved in 85% of the sample. mEHT toxicity was mostly mild (G1). The small total number of adverse events (5%) in this study supports the strong safety profile of mEHT. No complications were observed during the treatments. Cardiac evaluation was performed for all patients with EKG and echocardiography before and after the last cycle of mEHT. No significant variations were observed.
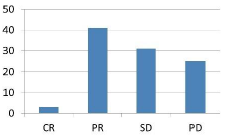
Figure 1. Tumor response (3 months)
Conclusion
mEHT appears to have promising efficacy in adults with several types of tumor and it can be considered as a highly indicated palliative therapy.
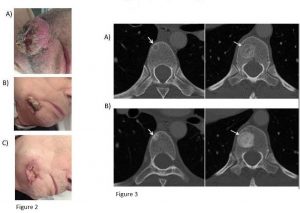
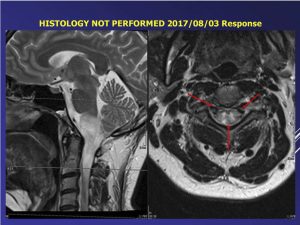
Figure 2. Patient with squamous cellular intraoral tumor
a) baseline, b) one and c) three months after mEHT.
The tumor arises from the gum and perforates the cheek.
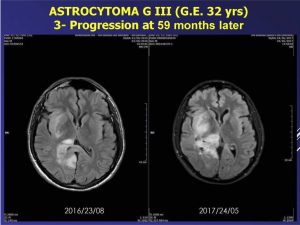
Figure 3. Patient, 49yrs with breast cancer and bone metastases.
a) CT scans at baseline showed partial osteolytic metastases (arrow) in thoracic vertebrae.
b) Three months after mEHT, osseous lesions din not change in size, but showed osteoblastic reaction (arrows in B), representing good response, and disappearance of the back pain.
Text extracted from Oncothermia Journal, Volumen 24, October 2018.
www.oncothermia-journal.com/journal/2018/Efficacy_of_Modulated_electro_hyperthermia_(mEHT)_in_cancer_ patients.pdf